|

Our early detection HIV test is able to detect HIV core antigen directly to bypass the need to wait for HIV antibody production by human body. This test is FDA approved but is very different from our regular antibody testing and usually offered and done in hospitals and required special licensing. We are proud to offer this to our patients for their peace of mind. Please refer to comparison table on this page for further information.
PEP
It stands for Post Exposure Prophylaxis. It means If you get exposed to HIV virus there is a short window period of 72 hours that under supervision of an experience doctor you could take special anti viral medicine. In this way your HIV infection might not get finalized and you increase your chance that you remain HIV negative !
The most effective methods for preventing human immunodeficiency virus (HIV) infection are those that protect against exposure to HIV. Antihero therapy cannot replace behaviors that help avoid HIV exposure (e.g., sexual abstinence, sex only in a mutually monogamous relationship with a non infected partner, consistent and correct condom use, abstinence from injection-drug use, and consistent use of sterile equipment by those unable to cease injection-drug use). Medical treatment after sexual, injection-drug--use, or other non occupational HIV exposure is less effective than preventing HIV infection by avoiding exposure.
Please refer to our PEP page link Click here
Window Period & Test Timing:
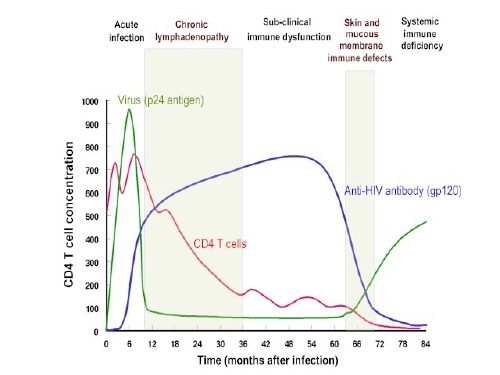
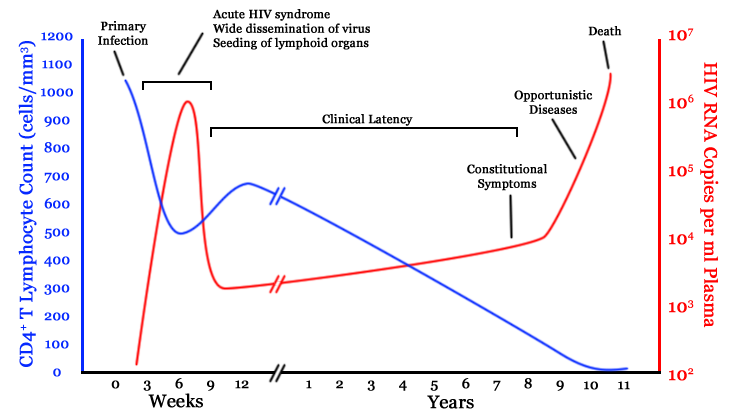
There are many tests available to detect HIV (EIA, Immunoassay, western blot, DNA PCR, Antigen testing, RNA PCR, quantitative viral load etc). The standard HIV test is a HIV antibody test. It will give you your HIV status (must always consider window period and future testing). It takes time for our body to produce antibodies against a HIV infection, so in the early acute phase of infection patients could be infected but the antibody test could come back negative. You must always test again in 6 months to confirm your result.
HIV Antigen Test
Main HIV test is HIV antibody test , antibody is what our immune system make against part of HIV which call antigen. By detecting HIV antibody against HIV antigen in the blood then that would be indicative there has been HIV presence. It is kind of indirect test. I give you example, It is like that you see the rain then you would imagine that there should be a cloud in the sky without looking and checking for cloud itself. Presence of rain indicative that there is a cloud.
Now, Think about detecting HIV antigen directly, If test detect HIV particle (antigen) directly then that is direct indicative of presence of HIV.. In afforemnetioned anology, this time you would look the sky to see the cloud and you don't need to wait for formation of the rain to verfy if there is cloud.
A) Pros : You can detect HIV faster brecause you are directly testing the HIV particle , as compare to HIV antibody test that you you need to wait longer period till immune system create antibody.
B) cons : Expensive, There might be wondow for HIV Antigen
HIV Antibody Test
It is what our body makes (special protein) against HIV (Ag) to fight against it. It takes some time that body produce antibody. The test will detect for antibody that our body produce. So indirectly we detect HIV , in other word, if you have antibody against HIV then you have the HIV. We are capable of checking for both HIV 1 and HIV 2 with blood in a few minutes. Our test is highly accurate, FDA approved, and done in our certified lab. We do not do home test or non-FDA approved self tests. An experienced medical doctor and not just a counselor will talk to you and answer all your specific questions. We will provide you with the official report with both the MD and Lab Director's signature the same day for your record, your doctor, or your partner.
We
use variety of test as follow in order to detect early HIV in our patients as follow:
1)Quantitates
HIV-1 virus RNA down to impressive 20 copies/mL (supersensitive) to monitor viral load in established HIV-1
infected individuals. (Specimens with viral loads greater than 10,000,000
copies/mL will be reported out as >10,000,000 copies/mL).
2)HIV Pro viral DNA Detects
the presence of HIV-1 Proviral DNA down to impressive 35 copies/million cells in peripheral
blood mononuclear cells that could potentially reactivate in HIV-1 positive
patients with undetectable viral loads (following antiretroviral therapy). Also
detects proviral DNA in individuals recently exposed to HIV but prior to
production of HIV-specific antibodies (including neonates of HIV-positive
mothers, accidental HIV exposure).
3)Quantitates
HIV-1 virus RNA down to 75 copies/mL to monitor viral load in established HIV-1
infected individuals (specimens with viral loads exceeding 500,000 copies/mL
will be run on dilution). Accurate for quantitation Group M subtypes (A-G)P24 Antigen.
4)P24 Ag is a protein product of the gag gene of HIV . As a viral, rather than host It appears with renewed viral replication. The reappearance of P24 antigen usually means progression to AIDS. Detection of P24 antigen could assist for early diagnosis of HIV as well.
5)Western Blot Separate HIV protein and glycoprotein in serum. This will detect various component such as Gp120/160 gp41 and etc.This test means to confirm HIV antibody positive patient of them being truly HIV positive in order to eliminate false positive test.
6)Viral load Test, It will check amount of the virus floating in serum, this will assist clinician to treat the patient with antiviral therapy and evaluate the progression and stage of the HIV.
7)Pool Sampling RNA, because an acute infection, prior to sero-conversion, is usually accompanied by high viral titers
(10E5-10E7), it is possible to identify viral NA with sufficient sensitivity in pools of >100 samples per test. This assay has been optimized to detect 1-5 copies/ml of HIV Viral RNA in a 512 specimen pool. The Sensitivity of tests per individual sample included in the pool is approximately 2000 copies/ml. This test has been approved for the screening of plasma product.
8)HIV antibody test will detect HIV 1/2 antibody in the body. There are many type of these tests available such as EIA, Immunoassay. It is the only FDA approved test for screening for HIV.
9) 4TH GENERATION HIV TEST, it is design to more accurately detect HIV upon screening. in family of HIV testing, 4th generation is the latest.
How Do We Do It ?
When you come to our center we will provide you with testing options and an explanation sheet. Then the doctor (MD) will answer all of your questions and discuss your testing options - We will take in to consideration of your time of exposure and your risk. Then consent will be obtained and test will be run. Doctor will give you your test result and speak with you about the result. You walk out with your official test report in few minutes.
| Comparison of Various Different HIV Testing Methode, Courtesy of Dr. S. Arani, M.D. Copyright protected |
Window Period |
False Negative |
Result Time |
Cost |
False Positive |
| HIV Immunoassay Blood Test |
4 weeks to 6 months |
Low |
15 Minutes |
++ |
++ |
| HIV EIA , Elisa |
4 weeks to 6 months |
High |
2-3 Days |
+ |
+++ |
| HIV Oral Test |
optimal in 3-6 Months |
High |
15 Minutes |
+ |
++ |
| HIV DNA PCR |
After 4 Weeks |
Low |
1 week |
+++ |
+ |
| HIV RNA |
Weeks to Months |
Low |
1-2 Days |
+++ |
+ |
| HIV Ultra S Ultra Q Nucleic Acid Testing |
Days |
Very Low |
3-7 Days |
++++ |
+ |
| Western Blot |
4 weeks to 6 months |
Low |
1 week |
+++ |
Low to none |
| Core Antigen Test |
14 Days |
Low |
30 minutes - 2 days |
+++ |
+ |
Above information and table is just for basic understanding and for our patient use only may not have diagnostic or therapeutic value.
HIV in Oral SEX
Risk of contracting HIV with unprotected oral sex is lower with vaginal and anal sex. However, it is just matter of time than you get contracted with HIV if you just keep doing it often enough. Duration of oral sex, presence of dental cavity, gum disease, having irriation in buccal mucosa or penile skin will all increase the risk of contracting HIV.
I give you one true example of my own patient story:
I had a patient who was coming to me for HIV test twice a year for at least 7 years and everytime he would give the resaon that he was doing HIV test because of his work and life insurance. His HIV test turning negative every single time. In one of his routine HIV test visit, he became positive, as I was in disbelief I run the test 3 times in my lab and everytime result turned out to be positive. It was difficult for me as I knew his family and had a great doctor-patient relation with him over many years. I enter the exam room to share the result but he found out from my facial expression before I spoke. He knew the routine is little different from his previous visits. He became emotional and it was then that he explained to me that all these years he has been visiting sex worker for oral sex and he has not been honest to me and been hidding that. He never had vaginal nor anal intercourse, but it was just matter of time that HIV infected him.
As human our exprience in life shape our view and judgment on daily basis. As a physicians, we are no different. We all go to medical school and post-graduate training, but what make us little different from one to other is our clinical experiences. I realized I have to put more emphasizes on oral sex risk. Telling patient that oral sex is "low risk" which we all learn might not be interpereted correctly. "Low risk" does not mean "no risk". Risk mutiplies and if you get involved in low risk activities multiple times or for long period then you gradually moving toward high risk group.
I give you another example, when you roll the dice the probability of getting number 6 is 1 out of 6 or 16.66 % now if you roll 2 dices the probability of getting 6 on each dice simultaneously is 1 in 36 which is 2.77 % .
If you roll dices many times (mutlipe oral sex contact, longer duration contact) then you increase your chance to see double six.
However, It is just a probability and mathematically they are independent value which means you could roll the dice once and on very first time you could get 6 on both . In other words, Low risk oral sex does not mean no risk and you still could get infected even with time or likley after many times. It does not worth it to risk of getting HIV for few moments of pleasure, so I always tell my patients to use protection for oral sex.
According to recent study and CDC
"Yes, it is possible for either partner to become infected with HIV through performing or receiving oral sex. There have been a few cases of HIV transmission from performing oral sex on a person infected with HIV. While no one knows exactly what the degree of risk is, evidence suggests that the risk is less than that of unprotected anal or vaginal sex.If the person performing oral sex has HIV, blood from their mouth may enter the body of the person receiving oral sex through
If the person receiving oral sex has HIV, their blood, semen (cum), pre-seminal fluid (pre-cum), or vaginal fluid may contain the virus. Cells lining the mouth of the person performing oral sex may allow HIV to enter their body. The risk of HIV transmission increases
-
if the person performing oral sex has cuts or sores around or in their mouth or throat; if the person receiving oral sex ejaculates in the mouth of the person performing oral sex; or
-
if the person receiving oral sex has another sexually transmitted disease (STD).
Not having (abstaining from) sex is the most effective way to avoid HIV."
PEP
It stands for Post Exposure Prophylaxis. It means If you get exposed to HIV virus there is a short window period of 72 hours that under supervision of an experience doctor you could take special anti viral medicine. In this way your HIV infection might not get finalized and you increase your chance that you remain HIV negative !
The most effective methods for preventing human immunodeficiency virus (HIV) infection are those that protect against exposure to HIV. Antihero therapy cannot replace behaviors that help avoid HIV exposure (e.g., sexual abstinence, sex only in a mutually monogamous relationship with a non infected partner, consistent and correct condom use, abstinence from injection-drug use, and consistent use of sterile equipment by those unable to cease injection-drug use). Medical treatment after sexual, injection-drug--use, or other non occupational HIV exposure* is less effective than preventing HIV infection by avoiding exposure.
How effective is this method:
There is no randomized, placebo-controlled clinical trial to check the true effectiveness of the treatment, and probably will never be a clinical trial because it is unethical to put people life at risk of HIV infection in order to test a drug. However, it seems to be effective . This approach is recommended by CDC and you could get more information on that from cdc.gov.
There are some data available from animal study and health care workers who got exposed with infected blood or HIV positive pregnant mothers who got similar approach which might sometimes reduce the risk for HIV infection after exposures by getting PEP.
Real Case Report:
I will give you 2 examples.
I tried it myself:
When I was doing my residency in MMC hospital in Phoenix Arizona, the big splash of blood scattered on my face while my intern was placing Swan-Gans cath in patient's chest. I was devastated and very afraid of getting HIV. At that time I was notified by hospital of post exposure prophylaxis (PEP) . I was given PEP medicine and fortunately I remained HIV negative by subsequent testing by my teaching hospital.
I gave it to my patient:
We received the phone call from a doctor who had sexual contact with a new partner which he met at a bar. After the sexual contact he noticed that his genitalia is contaminated with the girl's blood as she was menstruating. He became anxious and started questioning her just to find out that she was HIV positive. We initiated post exposure prophylactic treatment as last hope to protect him against HIV infection. He took PEP treatment recommended by us for one month and follow up for 6 months as he was finally declared as HIV negative. We could never find out what would be his HIV status if he had not taken PEP treatment, but that was the only option he had. One of the most important aspect of this example is that he was a doctor himself. HIV does not care about your status if you are poor, rich, prisoner or president. HIV is life changing syndrome it will impact your health, your financial status, your relationship and many other aspect of your life so use protection and get tested routinely and do not put yourself and public at danger.
Risk:
Blood transfusion > Needle Sharing injection Drug Use> Receptive Anal Intercourse > Precautions Needle stick > Receptive Penile Vaginal Intercourse > Insertive Anal intercourse > Incertive Penile-Vaginal Intercourse > Receptive Oral > Incertive Oral
HIV Testing:
Because persons who are infected with HIV might not be aware they are infected, baseline HIV testing should be performed on all persons seeking evaluation for potential HIV exposure. If possible, this should be done with an FDA-approved rapid test kit (we can do it in 15 minutes). If you are already HIV positive then you were not aware of it then maybe you do not need PEP and you need to be seen and follow up for your HIV treatment.
Is There Any Test to Detect HIV Exposure Before PEP ?
There is no test to detect HIV within first 72 hours after possible exposure. It makes sense because if there is chance to detect HIV in the blood then there is no benefit of PEP. The Whole Idea of PEP is to prevent HIV to enter the bloodstream. If HIV infect the blood then there is nothing you can do to reveres the course and become HIV negative again. Making HIV positive to HIV negative is ultimate cure that we don't have as of yet in practice of medicine in the world.
Follow ups:
If patient is candidate for Post exposure prophylaxis then candidate should have follow up evaluation and testing based on CDC recommendation. HIV medicine has risk and side effects and we need to check your liver, kidney and blood test to make sure the medicine is not effecting your health.
Our complete PEP management program will cover all these area till you get final test in 6 months to confirm your treatment has been successful and you are HIV negative.
Possible Early HIV infection Symptom (retroviral syndrome)
Fever , Headache , Tiredness, Enlarged Lymph nodes
Possible Later HIV symptom(before AIDS)
- Lack of energy
- Weight loss
- Frequent fevers and sweats
- Persistent or frequent yeast infections (oral or vaginal)
- Persistent skin rashes or flaky skin
- Pelvic inflammatory disease in women that does not respond to treatment
- Short-term memory loss
Window Period & Test Timing:
There are many tests available to detect HIV (EIA, Immunoassay, western blot, DNA PCR, Antigen testing, RNA PCR, quantitative viral load etc). The standard HIV test is a HIV antibody test. It will give you your HIV status (must always consider window period and future testing). It takes time for our body to produce antibodies against a HIV infection, so in the early acute phase of infection patients could be infected but the antibody test could come back negative. You must always test again in 6 months to confirm your result.
Compare Different HIV Test (Copyright protected
Dr. S. Arani ) |
Method |
Window Period |
Accuracy |
| HIV Antibody Test (first, second, third and fourth generation) |
Detection of human antibody against HIV antigen |
Weeks to Months , Maximum 6 months |
FDA approved
Blood test slightly more accurate than oral test. We use immunoassay blood test in our lab with result in 15 minutes |
| HIV Core Antigen Test |
Detection of HIV core antigen directly, (no need to wait for antibody production) |
Days to weeks |
FDA approved
Blood test , Result in 25 minutes in our lab |
| HIV Western Blot |
Detection variety of different antibody against HIV |
Weeks to Months |
FDA approved only for confirmation of positive HIV test and not for screening.
(you must have HIV positive test result by different method then your result will get confirmed by western blot to make sure your result is not false positive) |
| HIV DNA PCR |
Detection of HIV genetic information in infected blood |
Month to months
Not to be done in first 28 days after exposure |
Use for confirmation, during pregnancy, indeterminate western blot test result
|
| HIV RNA Qual |
Detection of HIV genetic information |
weeks to months
You could have HIV but in smaller number and your test become falsely negative |
Sometimes use for screening
but clinician has to be very carefully (consult your doctor, as case to case is different) |
HIV ultra S ultra Q RNA
|
Detection of quantity of HIV genetic information exist in blood |
Days
|
Difficult and technical test , not FDA approved for screening , but able to detect very minimal amount of virus in bloodstream |
| HIV RNA PCR quantitative |
Detection of quantity of HIV genetic information exist in blood |
Months to years |
Evaluation of HIV positive patients viral load |
Above information and table is just for basic understanding and for our patient use only may not have diagnostic or therapeutic value.
This must get explain by experienced physician for you.
HIV-2
HIV-2 is similar to HIV-1, the main difference is genetic information in RNA of the virus. Travelers to the Ivory Coast, Gambia, Nigeria, and Sierra Leon-if have been exposed to HIV, you may get a false negative test result in the USA If you just get checked for HIV 1. HIV-1 antibody test will not detect HIV-2 unless you inform your doctor and request a HIV-2 test as well.
For your convenience we have extended our phone lines
(323) 231-6000
(323) 231-7500
(323) 231-8200
(323) 231-7400
Welcome Walk-in
( Free Parking in Rear)
4524 S San Pedro Place
Los Angeles, CA 90011
|